
https://www.ncbi.nlm.nih.gov/books/NBK22301/
https://teamtelomere.org/diagnosis-management-guidelines/
Dyskeratosis congenita (DC) and other Telomere Biology Disorders are inherited conditions causing premature ageing due to telomere repair abnormalities. Telomeres protect the ends of our chromosomes and have been likened to the protective caps on the ends of shoelaces. Symptoms can include abnormalities of skin and nails, and in some cases, bone marrow failure (anaemia, low white blood count and platelet-blood clotting problems), or fibrosis (scarring) of lungs and liver cirrhosis.
The ‘Education’ tab on our home page has more details on symptoms affecting specific parts of the body. You can also find a list of ‘cheat sheets’ under the ‘Education’ tab – there is a sheet for each part of the body affected, as well as a general sheet that summarises all the symptoms. You may find it useful to print these off and show them to your GP or specialist doctor.
Who is affected?
Dyskeratosis congenita usually affects children and young people, but can occasionally affect older people. Dyskeratosis Congenita is diagnosed in one in a million. Other Telomere Biology disorders can cause symptoms later in life and affect several organs.
What is the cause?
Dyskeratosis congenita and other Telomere Biology Disorders are the result of mutations in telomere maintenance genes. Each time a cell divides, its telomeres get a little shorter. With ageing, cells divide many times. After many cell divisions, the telomeres become too short and the cell dies or functions abnormally. Depending on the type of cell, this may lead to medical problems, such as anaemia (when too many red blood cell producing cells have died) or lung / liver fibrosis (when minor lung or liver damage associated with day to day life heals with scarring) causing shortness of breath or cirrhosis.
Being born with a mutation in one of these genes doesn’t necessarily mean that you will have problems but you may be at increased risk. You may be able to minimize this risk by lifestyle modification.
Similarly, in some people who are diagnosed with with Dyskeratosis Congenita or a Telomere Biology Disorder, no genetic mutations can be found.
Other names for Dyskeratosis Congenita
Coats Syndrome, Coats plus Syndrome and Revesz Syndrome
CTC1& ST1 (Coats plus syndrome, DC and additional brain/retina(eye) calcification abnormalities) TINF2 (Revesz syndrome, similar to Coats plus, but also growth retardation, affecting babies & children) are associated with more severe disease.
Hoyeraal-Hreidarsson syndrome
Can be caused by any of the DC genes. This is a severe form of DC with abnormalities developing before birth, which include small brain (microcephaly), small cerebellum (brain balance centre and growth retardation. Affected children are small and have severe learning difficulties in addition to the other features of DC.
How is it inherited?
Currently the following genes are known to be associated with Dyskeratosis Congenita and Telomere Biology Disorders
TERT, TERC, PARN, RTEL1, NAF1, DKC1, NHP2, TINF2, NOP10, NHP2, ACD, RPA1, POT1, ZCCHC8 CTC1, DCLRE1B, NPM1, STN1, TCAB1, MDM4 and WRAP53
CTC1 (Coats plus syndrome, DC and additional brain/retina(eye) calcification abnormalities) and TINF2 (Revesz syndrome, similar to Coats plus, but also growth retardation, affecting babies & children) are associated with more severe disease.
Similarly, in some people with Dyskeratosis Congenita, no genetic abnormalities can be found.
The genes USB1 (C16orf57), GRHL2 and LIG4 are associated with DC-like symptoms, but not short telomeres.
Types of inheritance:
X-linked: DKC1
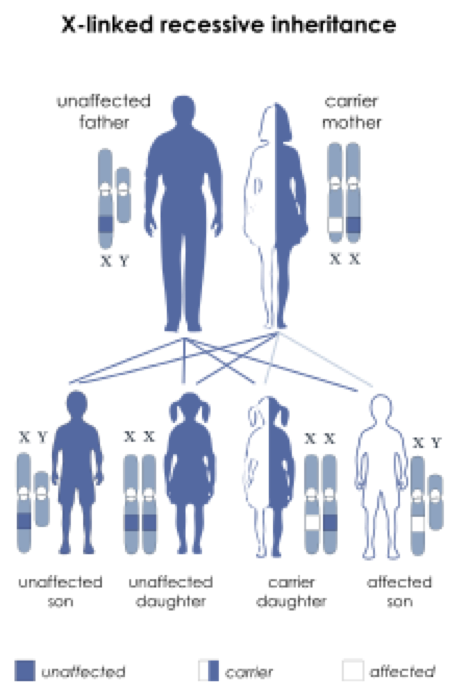
DKC1 gene mutations generally only affect males.
Females with an abnormal DKC1 gene are healthy carriers, their sons have a 50% chance of being affected and a 50% chance of being healthy/not carrying the gene. Their daughters have a 50% chance of being carriers- but will not have dyskeratosis congenita.
Males with an abnormal DKC1 gene are likely to be affected with dyskeratosis congenita. Their sons will be unaffected/not carry the gene, their daughters will be healthy carriers.
Autosomal recessive: TERC (some families), TERT (some families), RTEL 1 (some families), TINF2, PARN (some families), NHP2, NOP10
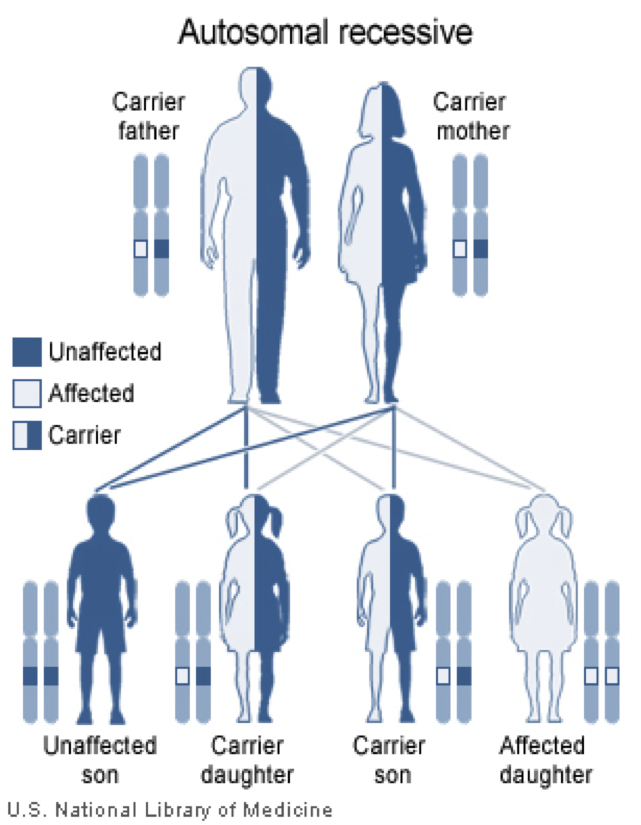
Two gene mutations (one from each parent) are generally required for dyskeratosis congenita. Parents who carry 1 gene mutation each have a 25% chance that each child will be affected.
Autosomal dominant: TERT (some families), RTEL1 (some families), PARN (some families)
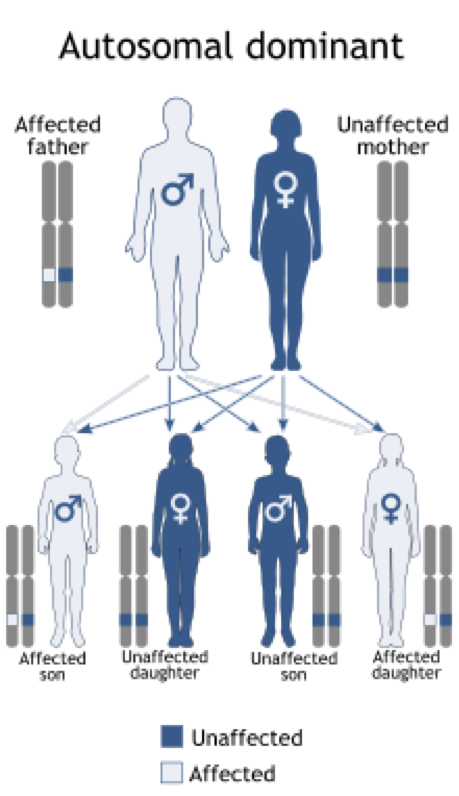
There is a 50% chance of each child of an affected person carrying the gene. Autosomal dominant genes generally are associated with onset of dyskeratosis congenita at an older age, sometimes in old age, and some people remain healthy.
If you have any questions, please contact our medical advisor, Dr. Hilary Longhurst.
You can listen to Dr. Longhurst’s presentation at the August 2018 Cambridge Rare Disease Showcase below:
You can hear a medical overview of Dyskeratosis Congenita on the Instagram post
Medics for Rare Diseases – an overview of Dyskeratosis Congenita
Disclaimer: The materials contained on this website are provided for general information and guidance purposes only, and do not constitute advice in their own right. For medical advice, please contact your doctor.